Haemolytic uraemia syndrome (HUS) is a form of microangiopathic haemolytic anaemia (MAHA). MAHA refers to a subgroup haemolytic anaemia, in which red cells are destroyed, by factors in the capillaries. These include the deposition of fibrin and endothelial damage.
Atypical Hemolytic Uremic Syndrome (aHUS) and Typical Hemolytic Uremic Syndrome (tHUS) are both rare but serious conditions characterised by a triad of symptoms, including microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury. However, these syndromes differ in their underlying causes and clinical presentations. Atypical HUS is primarily associated with dysregulation of the complement system, an important part of the immune system, leading to uncontrolled activation and damage to blood vessels. It often manifests without a preceding diarrheal illness, which is a hallmark of tHUS. Genetic mutations, acquired factors, and complement dysregulation contribute to the development of aHUS, making it less predictable and potentially more challenging to manage.
On the other hand, tHUS is typically triggered by infections, most commonly those caused by certain strains of Escherichia coli bacteria, such as the Shiga toxin-producing E. coli (STEC). These infections are often foodborne and can result in gastrointestinal symptoms before progressing to the triad of symptoms seen in HUS. tHUS is more prevalent in children and is often associated with outbreaks, such as those linked to contaminated food or water sources. While both aHUS and tHUS share overlapping clinical features, their distinct etiologies necessitate different approaches to diagnosis and management, highlighting the importance of accurate differentiation for appropriate medical intervention.
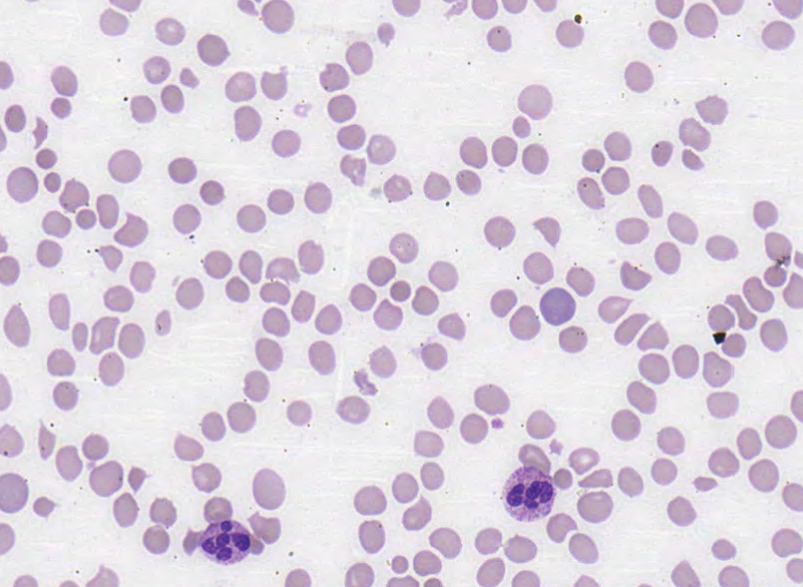
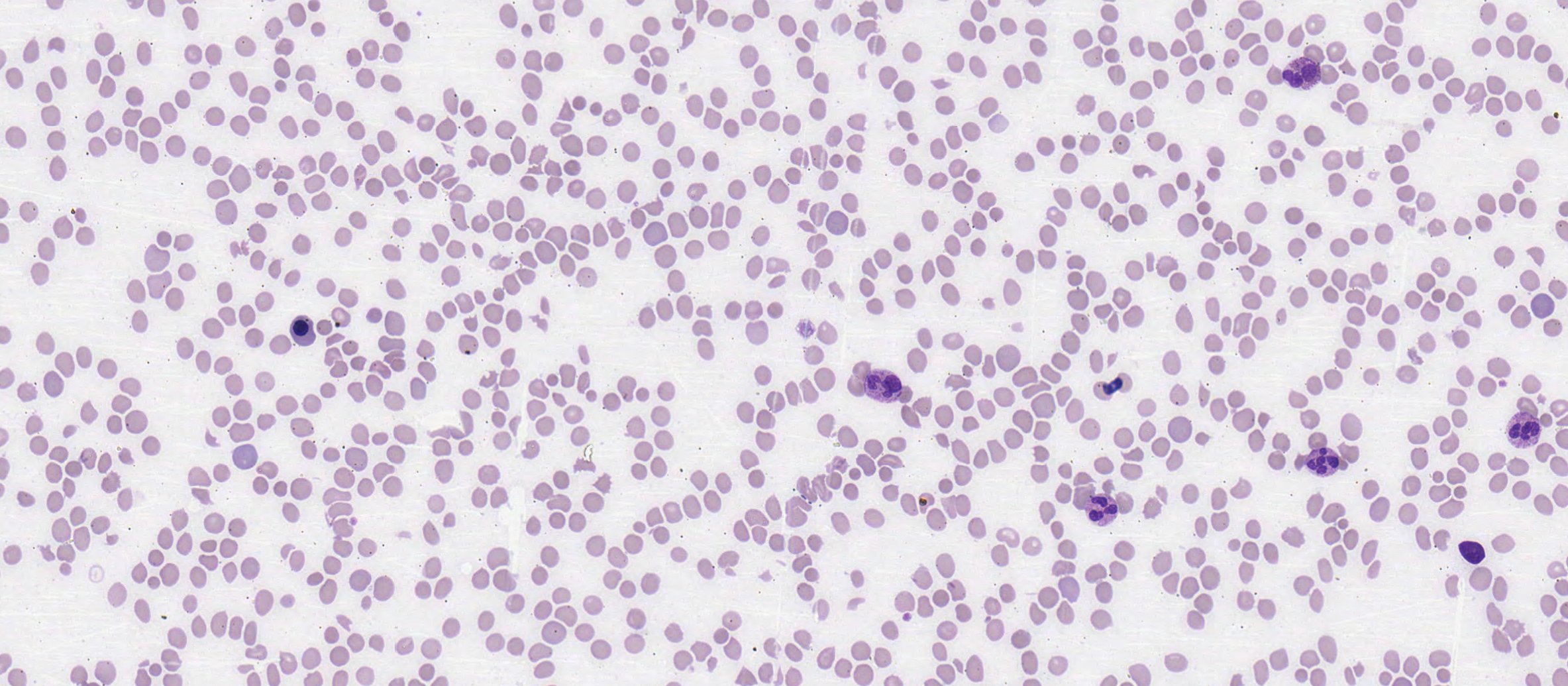
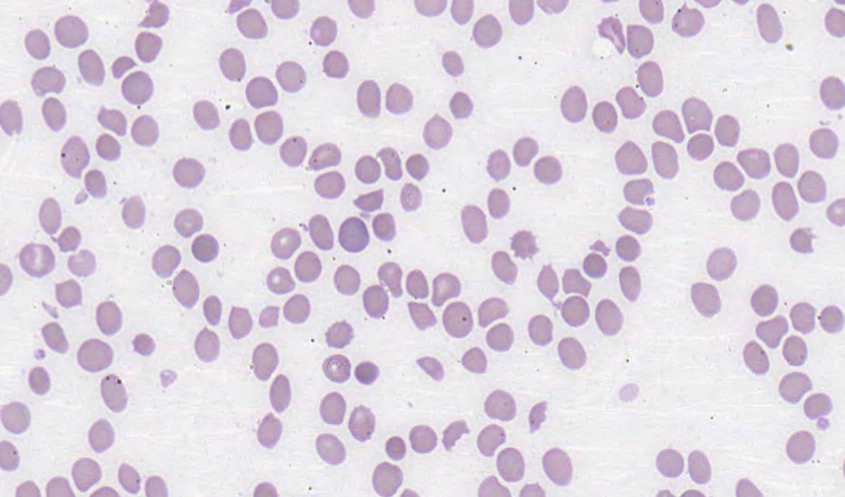
Features of HUS on the peripheral blood film:
- Red cell anisocytosis
- Red cell fragment
- Microspherocytes
- Polychromasia
- Thrombocytopaenia
- Nucleated red cells
_____
Images from personal photography.