Thank you to everyone who analysed the images for our NICU mystery. Before we reveal the diagnosis, let’s look at the “evidence list” that led us there.
The Blood Film Features:
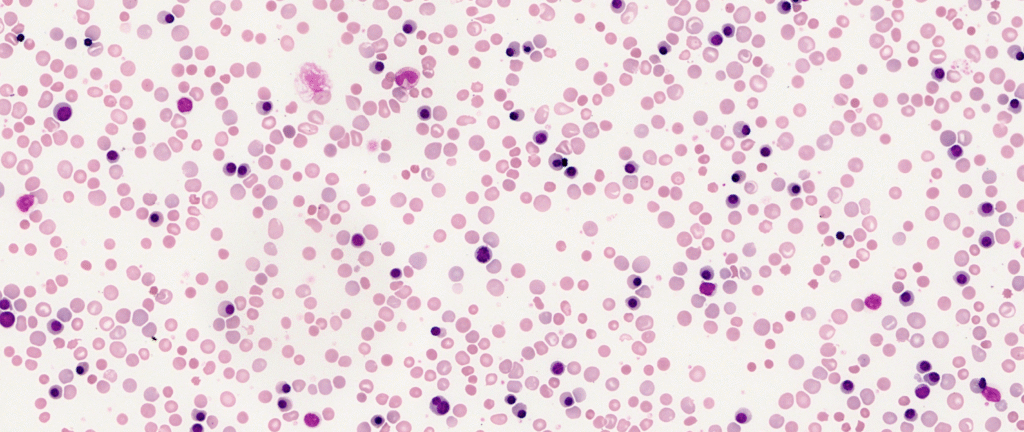
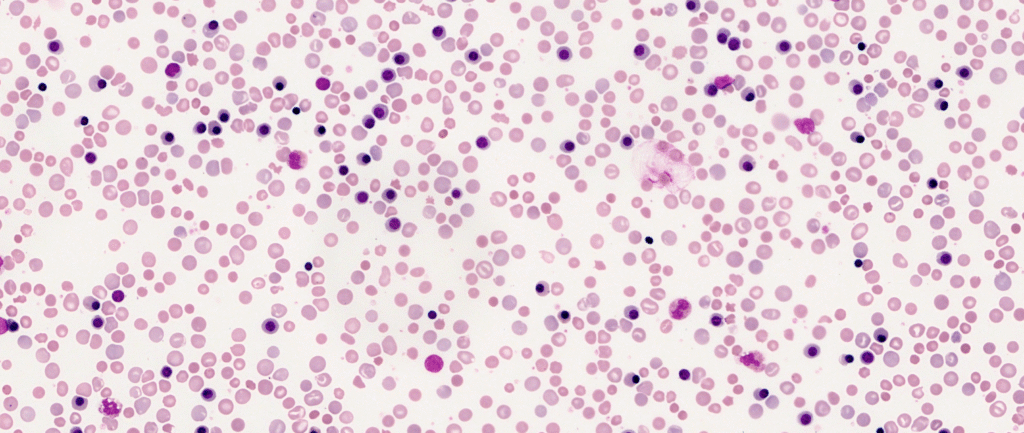
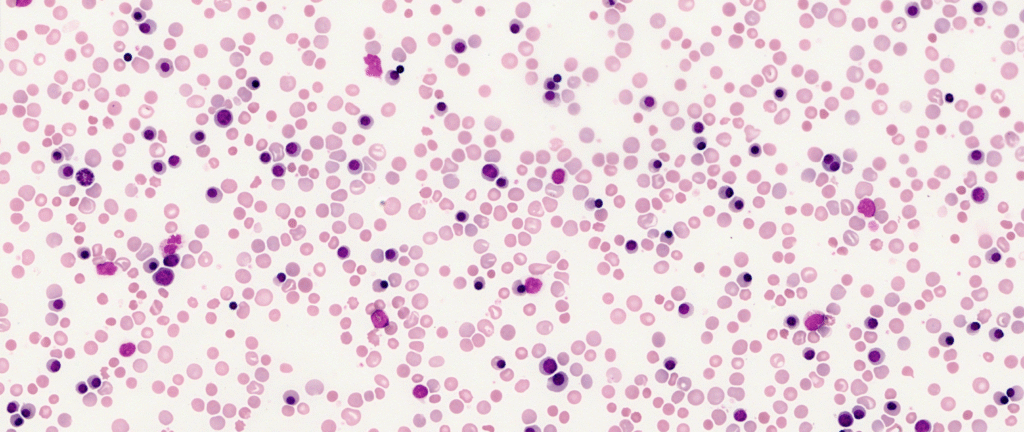
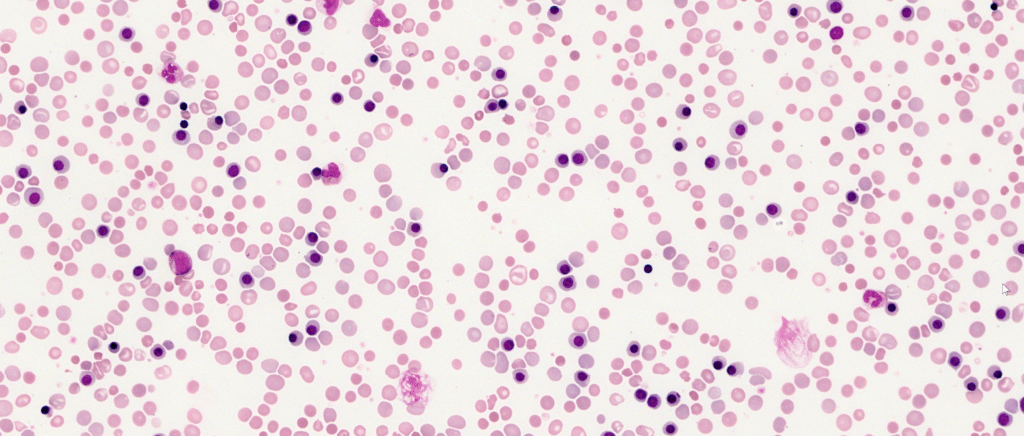
Under the microscope, this neonate’s blood film was anything but “quiet.” It showed a classic hyper-regenerative picture:
- Spherocytes: Small, dense red cells lacking central pallor, indicating that maternal antibodies are causing splenic macrophages to “nibble” at the red cell membranes.
- Prominent Polychromasia: A high number of large, grey-blue immature red cells, showing that the bone marrow is responding vigorously to the anaemia.
- Circulating Nucleated Red Blood Cells (NRBCs): These precursors are being pushed out into the circulation prematurely due to the extreme erythropoietic stress.
The Diagnosis: HDFN due to Rh Sensitisation (Anti-D)
Based on these findings, the diagnosis is Haemolytic Disease of the Foetus and Newborn (HDFN) caused by Rh sensitisation, following the clinical scenario where the mother did not receive anti-D prophylaxis.
Why the Morphology Rules Out Kell
While both Rh and Kell antibodies can cause severe neonatal anaemia, they look completely different on a blood film.
In Rh sensitisation, the antibodies target mature red cells in the circulation. The bone marrow remains unaffected and reacts by working overtime to replace the destroyed cells, hence the abundance of NRBCs and polychromasia.
In contrast, Kell-induced HDFN is primarily a disease of marrow suppression. Anti-Kell antibodies target and destroy erythroid progenitor cells (the “babies” of the red cells) before they can even develop.
If this had been an anti-Kell case, the film would have been hyporegenerative. Despite a low haemoglobin, you would likely see a “deathly quiet” film with an unexpected absence of polychromasia and NRBCs.