Thank you to everyone who participated in this week’s sobering case. The green inclusions noted in the neutrophils of our ICU patient are a rare and clinically critical finding.
“Crystals of death”

These inclusions are formally known as critical green inclusions or green neutrophilic inclusions. In clinical circles, they have earned the ominous nickname “crystals of death” due to their strong association with impending mortality.
A review of documented cases reveals a consistent and striking pattern:
- Prognostic Significance: These crystals are considered a “critical result”. Historically, their appearance has been linked to a very high short-term mortality rate, with some studies reporting that up to 65% of patients expire within 72 hours of the inclusions being identified on a blood film.
- Clinical Associations: They are most frequently identified in the setting of acute liver failure, fulminant hepatic injury, or severe lactic acidosis. However, recent literature has also noted them in cases of septic shock, ischemic bowel disease, and multi-organ failure.
- Biochemical Composition: While once thought to be phagocytosed bile products (like biliverdin), more recent studies using special stains (such as Oil Red O) and electron microscopy suggest they are actually lipofuscin or lipofuscin-like deposits. These likely represent lysosomal degradation products resulting from catastrophic tissue or liver injury.
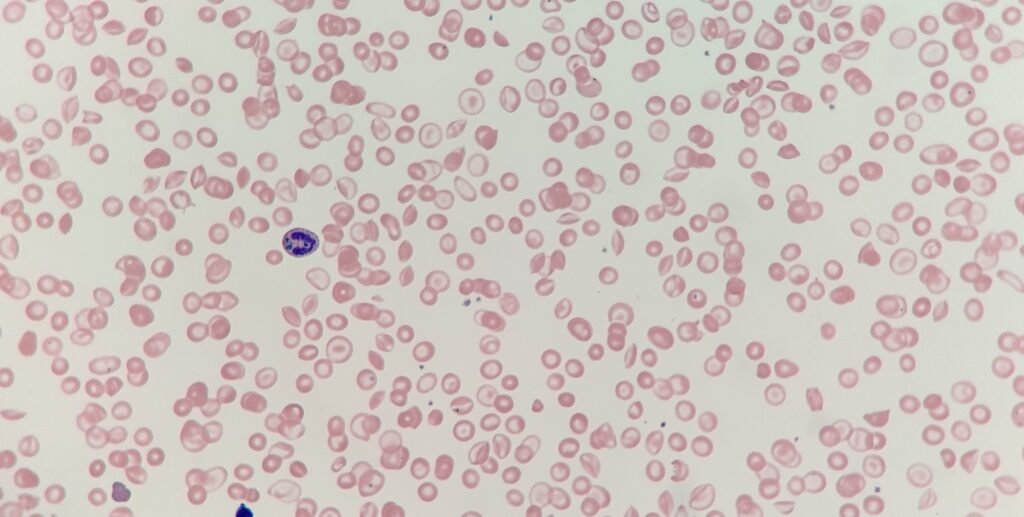
Associated morphology:
In addition to the “death crystals,” patients in liver failure often exhibit distinct red cell changes, including:
- Acanthocytes (spur Cells): These irregularly thorny cells develop when severe liver disease causes free cholesterol to accumulate in the plasma and insert into the red cell membrane, increasing the cholesterol-to-phospholipid ratio and creating a rigid, misshapen structure that is further remodelled by the spleen.
- Target Cells (codocytes): This “bullseye” appearance occurs because obstructive liver disease inhibits the enzyme LCAT, leading to an absolute increase in membrane cholesterol and lecithin; this expands the surface area relative to the cell volume, causing the membrane to flatten and fold in on itself.
- Macrocytosis: A raised MCV is frequently seen in hepatic failure because the physical deposition of lipids expands the cell membrane, while simultaneous “stress” erythropoiesis releases larger, immature reticulocytes into the circulation even in the absence of B12 or folate deficiency.
While the nickname “crystals of death” is daunting, some recent case series suggest that recovery is possible if the underlying cause (such as ischemia) is reversible. However, their presence should always trigger an immediate “red flag” for the clinical team, indicating that the patient is in a state of extreme physiological stress.